60Y old male with sob, abdominal distention and bilateral pedal edema since 4 days
Patient came with chief complaints of shortness of breath since 4 days, pedal edema since 4 days and abdominal distention since 4 days
Patient was apparently asymptomatic 5 years back when he had an injury to the left leg by a thorn prick for which doctor advised him to keep ice over it. He did this for 5 days when he noticed swelling accompanied by blebs. Swelling was localised and associated with pain which was non radiating, no know aggravating or releiving factors for which he was admitted and dressing was done for 1 week and later ok discharged after the swelling had reduced. During this visit to the hospital he was given a pint of blood transfusion due to decreased heamoglobin count.
The patient complains of neck pain from 10 years has history of lifting heavy weights on shoulders, non radating, no known aggravated and releving factors. Some releif on using collar. Use it when he is unable to bear it. H/o knee pain since 10 years bilateral non radiating aggravates on walking relieves on taking rest. The patient had a history of similar complaints 6 months back where he had been admitted to the hospital and upon investigations found that he had low haemoglobin (hb 6) and was tranfused with a pint of blood and sent back to home
1 month ago he developed cough which was insidious in onset gradually progressive no known aggravating factors relieved on medication after 8 days. Cough was associated with sputum whitish in colour scanty in amount relieved with cough on medication.1 week back he developed dry cough insidious in onset non progressive releived on medication. The patient was alright 4 days back then he developed shortness of breath insidious in onset gradually progressed from grade 1 to grade 4 in 4 days no orthopnea, no pnd
He developed pedal edema from 4 days which was insidious in onset progressed from bilateral ankle to below knee, pitting type of edema no decreased urine output not associated with facial puffiness.
He also complained of abdominal distention since 4 days associated with easy fatiguability
No H/O excessive sweating, chest pain, palpitations
No H/O nausea, vomiting, abdominal pain, diarrhea
No H/O fever, cough, cold
Complains of constipation since 10 days
Past history:-
Similar complaints 6 months ago relieved on medication and blood transfusion
Known case of diabetes since 10years on tab metformin 500 mg and tab glimiperide 2 mg po/od
Not a known case of hypertension epilepsy, TB CVA CAD
Personal history
Sleep adequate
Addictions alcohol since 30 years every day 90 ML
Addictions of tobacco since two years
Bowel and bladder movements regular
GENERAL EXAMINATION
Patient is conscious coherent and cooperative
Pallor present
Clubbing absent
Icterus absent
Pedal edema present
Lymphadenopathy absent
Cyanosis absent






SYSTEMIC EXAMINATION
CVS S1 S2 heard no murmurs
RESPIRATORY bilateral air entry present non vesicular breath sounds heard
CNS no focal neurological deficits
Per abdomen
On examination
Distended
shifting dullness present
INVESTIGATIONS
08/12/24












09/01/24





10/01/24
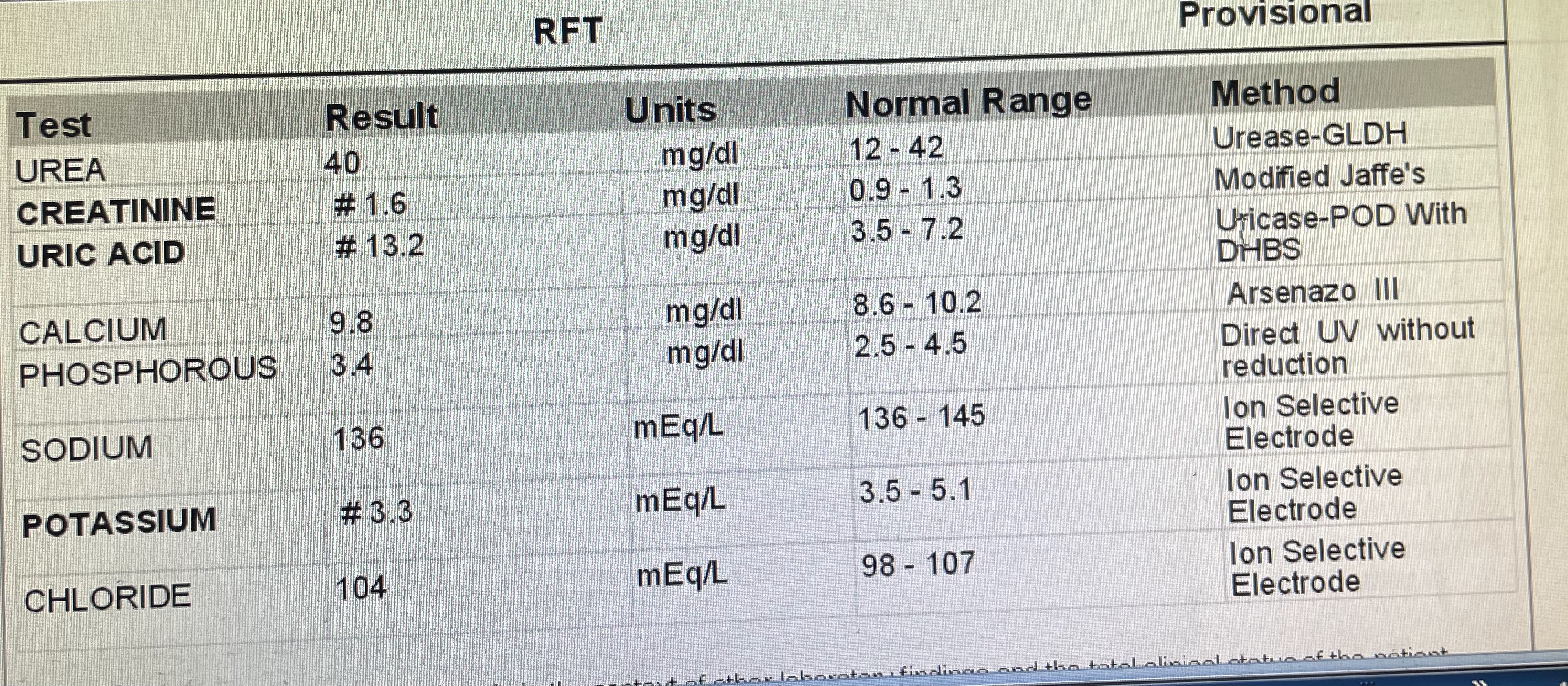

11/01/24

TREATMENT GIVEN
DAY-1 08/01/24
IRON RICH DIET
INJ.LASIX 40mg IV/STAT
INJ.IRON SUCROSE 200MG+100MG NS/IS/OD
TAB.OROFER-XT PO/BD
TAB.NEUROKIND-LC PO/OD
TAB.LIMCEE PO/OD
TAB.CARVEDILOL 3.125MG PO/OD
DAY-2 09/01/24
IRON RICH DIET
INJ.LASIX 40mg IV/BD
INJ.IRON SUCROSE 200MG+100MG NS/IS/OD
TAB.OROFER-XT PO/BD
TAB.NEUROKIND-LC PO/OD
TAB.LIMCEE PO/OD
TAB.TELMA 20MG PO/OD (changed from carvedilol)
INJ.VITCOFOL 2CC IM/OD(added)
INJ.THIAMINE 200MG IN 100ML NS IV/OD(added)
INJ.HUMAN ACTRAPID INSULIN SC/TID(added)
BLOOD TRANSFUSION DONE- NO REACTIONS OBSERVED
DAY-3 10/01/24
IRON RICH DIET
INJ.LASIX 40MG IV/BD
INJ.IRON SUCROSE 200MG+100MG NS/IS/OD
TAB.OROFER-XT PO/BD
TAB.NEUROKIND-LC PO/OD
TAB.LIMCEE PO/OD
TAB.TELMA-H 40MG/12.5MG PO/OD (changed from telma 20mg)
INJ.VITCOFOL 2CC IM/OD
INJ.THIAMINE 200MG IN 100ML NS IV/OD
INJ.HUMAN ACTRAPID INSULIN SC/TID
BLOOD TRANSFUSION DONE- NO REACTIONS OBSERVED
DAY-4 11/01/24
IRON RICH DIET
INJ.LASIX 40MG IV/BD
INJ.IRON SUCROSE 200MG+100MG NS/IS/OD
TAB.OROFER-XT PO/BD
TAB.NEUROKIND-LC PO/OD
TAB.LIMCEE PO/OD
TAB.TELMA-H 40MG/12.5MG PO/OD
INJ.VITCOFOL 2CC IM/OD
INJ.THIAMINE 200MG IN 100ML NS IV/OD
INJ.HUMAN ACTRAPID INSULIN SC/TID (8U bbf — 8U bl — 8U before dinner)
TAB.GOODCEF-CV 200MG BD (added)
INJ.NPH SC BD (4U bf — 4U before dinner) (added)
DIAGNOSIS
MICROCYTIC HYPOCHROMIC ANEMIA SECONDARY TO ?IDA
(?HEART FAILURE SECONDARY TO ANASARCA)
TYPE 2 DM SINCE 10 YEARS



Comments
Post a Comment